What the UHC Prior Auth Expansion Means for Your PT and Chiropractic Billing Team
UHC's Medicare Advantage prior authorization program keeps expanding. Here's what the 6-visit waiver actually covers — and where the documentation traps are.
UnitedHealthcare's Medicare Advantage prior authorization program for outpatient therapy and chiropractic services keeps expanding, and the operational burden lands on billing teams. Arizona and California were added effective February 1, 2026. For practices not yet in an expansion state, the question is workflow readiness — the requirement is arriving on a known trajectory.
Knowing what the expansion actually requires, and where the documentation traps are, is what separates practices that absorb the change from practices that absorb the denials.
The Policy Shift Every Billing Manager Needs to Understand
UHC's Medicare Advantage PA program for outpatient therapy and chiropractic has been rolling out nationally since September 2024. The program requires prior authorization for physical therapy, occupational therapy, speech-language pathology, and chiropractic services under covered Medicare Advantage plans. The initial evaluation is exempt — patients can be evaluated without PA — but ongoing care generally requires an approved plan of care before treatment proceeds.
The workflow implication is immediate. A practice managing UHC Medicare Advantage patients across multiple providers needs a reliable system for tracking which visits require authorization, which have approvals in hand, and when plans of care need renewal. Without that, claims submit without valid authorization and denials follow.
The "6-Visit Waiver" — What It Covers and What It Doesn't
UHC's program includes a clinical review waiver: the first six visits of an initial plan of care are covered without clinical review, provided they're delivered within eight weeks of the initial evaluation (UHCprovider.com provider bulletin; APTA coverage, 2026).
The waiver reads like relief, but it's a documentation layer that still requires active tracking.
The waiver applies to the initial plan of care, not subsequent ones. Once a patient moves into ongoing care — or returns after a gap — those conditions may not apply. And "without clinical review" doesn't mean without prior authorization. UHC still requires authorization; it simply waives the clinical documentation requirement for those first six visits when conditions are met.
Billing teams that read this as "no prior auth for the first six visits" are likely to discover the error at the denial stage. The administrative burden hasn't been lifted — it's been structured differently. Knowing the difference before submission matters considerably more than learning it after.
Why Northeast Practices Should Be Watching Now
If your practice is in the Northeast, you're not yet in the expansion window — but the trajectory is clear. State-by-state rollout is how this kind of PA program spreads, and practices that wait until the requirement arrives to build a workflow are already starting behind.
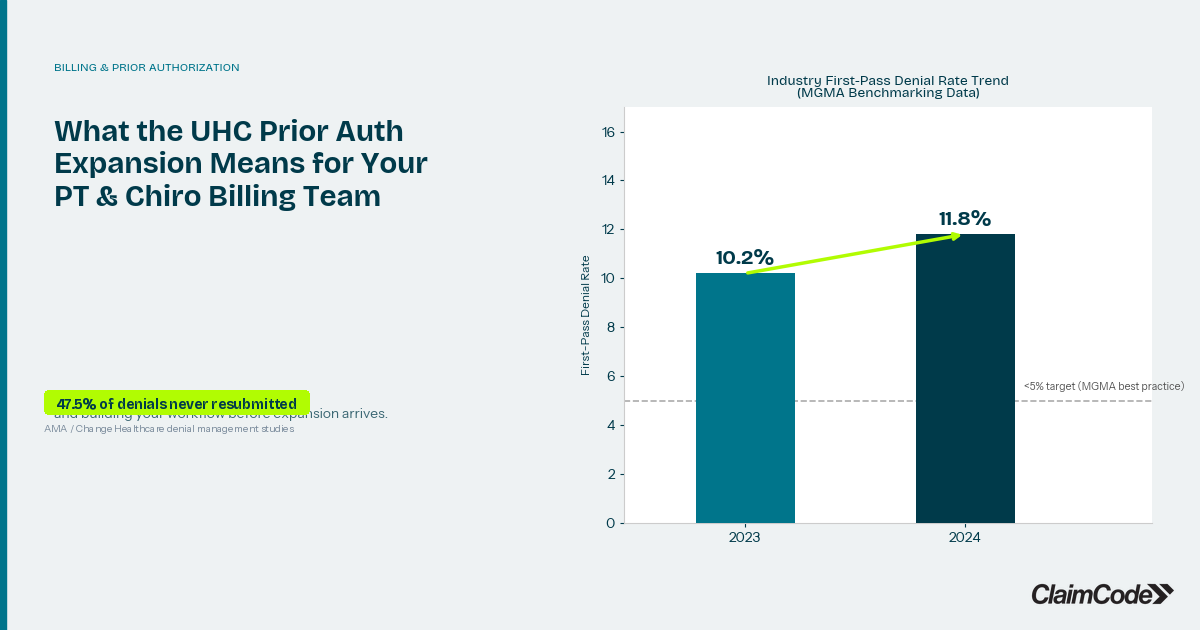
Claim denial rates have been climbing. MGMA's most recent benchmarking data shows first-pass denial rates reached 11.8% in 2024, up from 10.2% the prior year. Prior authorization failures are one of the fastest-growing denial categories for outpatient therapy. Adding a PA-required payer without a documented internal process is a reliable path to a denial spike — not because the billing team did anything wrong, but because the requirements weren't surfaced early enough to prevent it.
The practices that handle prior auth without significant denial exposure do it by building visibility into which claims have authorization in hand before the date of service — not by adding headcount.
The Real Revenue Cost of Prior Authorization Burden
Prior authorization isn't just an administrative inconvenience. It's a documented source of revenue leakage.
When PA requirements aren't tracked cleanly, the chain is predictable: claims submit without authorization, denials issue, and billing teams absorb an appeal queue on top of their routine workload. Wellness practices already spend 20 to 30 hours per month on manual claim follow-up, according to APTA administrative burden studies. Prior auth denials add to that total.
And the math on unrecovered denials isn't favorable. AMA and Change Healthcare data shows that 47.5% of denied wellness claims are never resubmitted — not because billing managers don't intend to follow up, but because without clear prioritization, some denials fall out of the queue. Change Healthcare's 2024 revenue cycle data puts average annual revenue leakage at $80,000 to $100,000 per practice. Prior auth failures are a compounding contributor to that number.
The system has added administrative complexity that practices had no role in designing. The financial consequence still lands on the practice.
A Federal Rule That's Supposed to Help — But Not Yet
CMS's prior authorization and interoperability rule (CMS-0057-F), with compliance requirements taking effect in 2026, requires insurers to respond to urgent PA requests within 72 hours and standard requests within seven days, and mandates electronic prior authorization processes.
This is a real shift in the right direction. It creates response-time standards payers haven't always honored and electronic workflows that cut down on manual back-and-forth.
The operational relief won't arrive uniformly or immediately. Compliance timelines vary across health plans, and the technology infrastructure on both sides needs time to catch up. For billing managers in 2026, prior auth workflows still require close, current attention. The rule changes the long-term picture, not today's queue. When payer processes do improve, practices with strong PA tracking will absorb the change without disruption. Practices relying on manual follow-up will capture less of the benefit.
What Billing Teams Can Do Now
Prior authorization management is a workflow problem before it's a technology problem. A billing team that knows, at the start of each week, which scheduled patients have active authorizations and which need PA submitted before the date of service is operating from a position of control. A team discovering the authorization gap at claim submission is not.
The starting point is visibility: a current picture of PA requirements by payer, authorization status by patient, and a reliable process for flagging renewals before they lapse. Most billing teams have pieces of this information — distributed across EHR notes, spreadsheet trackers, and the institutional memory of the person who manages that payer relationship. Making it consistent and accessible is what prevents the gaps from becoming denials.
If your practice sees UHC Medicare Advantage patients and isn't yet in an expansion state, now is the time to build the workflow. The expansion is a when, not an if.
To talk through how ClaimCode tracks prior authorization status and surfaces denial risk for your specific payer mix, book a meeting with our team at claimcode.app/contact.
Related Reading
Denied Outpatient Claims Rose 14% in 2025. Here's What That Costs the Average PT or Chiro Practice.
Denied outpatient claim amounts rose 14% in 2025. Here's what the math means for PT and chiro practices — and how to stop the revenue from walking out the door.
ERA Reconciliation for Physical Therapy Practices: What the Data Is Trying to Tell You
Most PT practices post ERA payments without reading the patterns underneath. Here's what your remittance data reveals — and what it's costing you.

Dr. Andrew O'DonnellPhD, LSSGB
CEO and founder of ClaimCode. Expert in insurance analytics, digital transformation, and business operations. Passionate about helping private wellness practices manage their revenue cycle with meaningful insights.
Ready to stop losing revenue to denied claims?
ClaimCode gives your billing team real-time claim visibility and AI-powered remediation guidance — at flat-fee pricing.
Get Early Access