Denied Outpatient Claims Rose 14% in 2025. Here's What That Costs the Average PT or Chiro Practice.
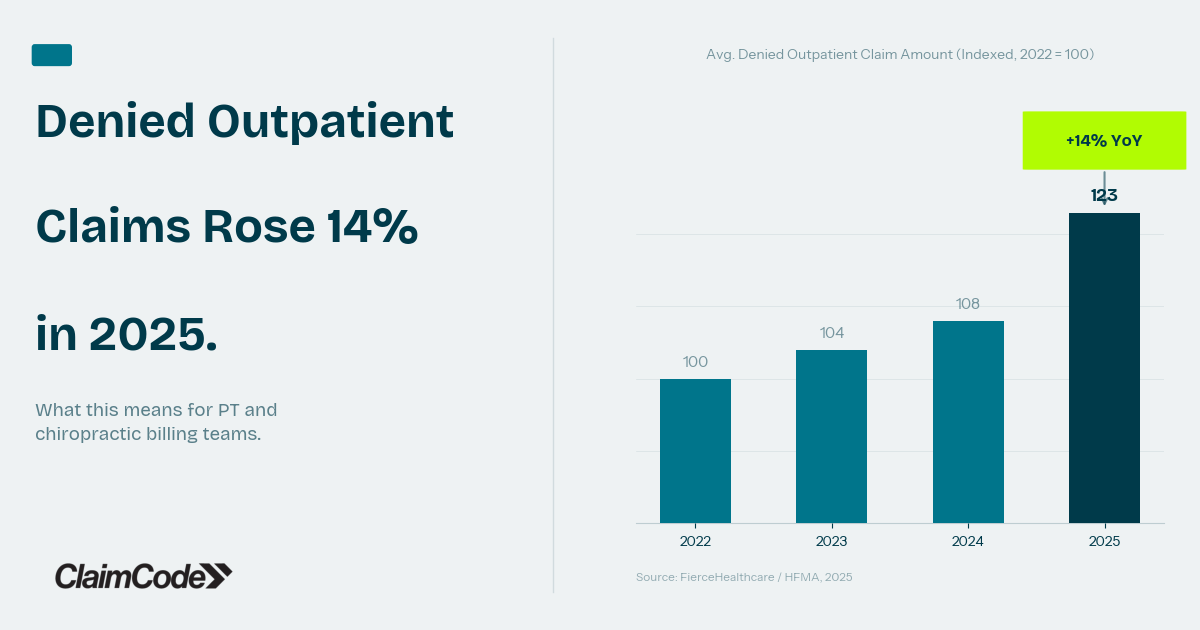
Denied outpatient claim amounts rose 14% in 2025. Here's what the math means for PT and chiro practices — and how to stop the revenue from walking out the door.
Somewhere in the revenue cycle of the average outpatient therapy or chiropractic practice, money is leaving through a gap that most billing teams can measure but few can fully close. In 2025, the average denied outpatient claim amount rose 14% compared to the prior year — across a network of 1.2 million providers tracked by FierceHealthcare and HFMA. That figure isn't about denial rates. It's about the dollar value of every denied claim, and how that number is climbing even when submission volumes hold steady. For billing managers already working through a dense queue of payer requirements, a 14% rise doesn't feel like a trend report. It feels like a Tuesday.
The 14% Number and What It Actually Measures
Most billing teams track denial rate — the percentage of submitted claims that return denied. It's a useful metric. But denial rate alone can mask a more expensive pattern: when the claims being denied are higher-value, the revenue impact compounds faster than the rate would suggest.
A practice with a 10% denial rate is already above the MGMA benchmark target of under 5% for high-performing practices. But if that 10% is concentrated in complex visits, extended evaluations, or multi-unit CPT codes, the revenue consequence is considerably larger than a simple percentage implies.
The FierceHealthcare data captures this distinction. The 14% rise in denied outpatient claim amounts reflects a payer environment in which clinical review criteria are tightening precisely where services are most clinically intensive — and most expensive to re-work. Practices aren't just dealing with more denials. They're dealing with bigger ones.
Why Payer Scrutiny Is Concentrating on Outpatient Therapy
The increase in denied claim amounts isn't random. Payers have been systematically tightening clinical review criteria for outpatient therapy and chiropractic services, particularly under Medicare Advantage. Prior authorization expansion programs currently rolling out in multiple payer networks are one visible example, but they're part of a broader pattern: payers directing audit and clinical review resources toward service categories with high utilization and reimbursement rates.
MGMA's benchmarking data shows that more than half of U.S. healthcare organizations now report denial rates exceeding 10%, with first-pass denials rising from 10.2% to 11.8% between 2023 and 2024. The practices being hit hardest aren't failing at billing. They're encountering a payer environment that has added layers of scrutiny without adding comparable documentation guidance or response-time accountability.
The system has added complexity. The cost of that complexity lands on the practice.
The Compounding Math of Unrecovered Denials
Here's where the 14% increase in denied claim amounts becomes a real number for a real practice: most denied claims are never recovered.
AMA and Change Healthcare denial management studies estimate that 47.5% of denied wellness claims are never resubmitted. Separately, 65% of denials are never appealed at all. Those figures aren't indictments of billing teams — they reflect the practical reality of a workflow where appeals require time, payer-specific knowledge, and documentation that isn't always surfaced at the moment it's needed.
Change Healthcare's 2024 revenue cycle analytics put average annual revenue leakage per wellness practice at $80,000 to $100,000. That number is driven by outright write-offs, underpayments that go unchallenged, and denials that age out of the appeal window before anyone gets to them. When the dollar value of each denied claim rises, leakage at the same recovery rate produces larger losses.
Where the Money Goes When a Claim Doesn't Come Back
Denied claims that aren't recovered don't disappear cleanly from a practice's balance sheet. They move through a predictable path: denied, entered into a follow-up queue, partially worked, then aged past the appeal window or written off when the time investment no longer makes sense.
Wellness practices already spend 20 to 30 hours per month on manual claim follow-up, according to APTA administrative burden studies. That time is spread across routine remittance reconciliation, authorization tracking, and denial management. When denial amounts rise, the same hours produce less recovery — not because the billing team is less capable, but because the workload has grown without a proportional increase in visibility into which denials are still worth pursuing and which have already crossed into write-off territory.
The $262 billion in denied claims processed annually across U.S. healthcare represents the aggregate of individual practices making that same calculation in real time, often without complete information (Change Healthcare 2024 Revenue Cycle Analytics).
What Practices with Lower Leakage Are Doing Differently
Practices that consistently recover a higher share of denied revenue share a common characteristic: they have current, actionable information about their denial patterns before claims age out.
HFMA's denial prevention best practices cite a 54% recovery rate when denials are properly appealed and resubmitted — versus near-zero recovery for claims that age past the appeal deadline without action. The gap between those two outcomes is almost entirely about timing and visibility. A billing team that knows, at the start of each week, which denied claims have viable appeal paths and which are at risk of aging out can make decisions. A team discovering denial details at the write-off stage can't.
The practices absorbing a 14% increase in denied claim amounts with less revenue impact aren't necessarily adding billing headcount. They're working from a clearer picture of where their denial dollars are going — and which ones are still recoverable.
Building Denial Visibility Before It Becomes Revenue Loss
Improving denial recovery starts with building a clear view of your practice's denial economics: what's being denied, at what dollar value, by which payers, and at what stage in the appeal cycle. Practices with that visibility can prioritize follow-up on high-value denials before they age out, identify payer-specific patterns that point to a billing process problem rather than a one-off claim, and stop absorbing write-offs that were avoidable with better timing.
The 14% rise in denied outpatient claim amounts is a payer-side trend that no individual practice controls. But the recovery rate — how much of that denied revenue comes back — is a function of internal process and visibility. That part practices can improve.
If you're ready to get a clearer picture of your practice's denial economics, ClaimCode is now accepting early access requests. Join the waitlist at claimcode.app.
Related Reading
What the UHC Prior Auth Expansion Means for Your PT and Chiropractic Billing Team
UHC's Medicare Advantage prior authorization program keeps expanding. Here's what the 6-visit waiver actually covers — and where the documentation traps are.
ERA Reconciliation for Physical Therapy Practices: What the Data Is Trying to Tell You
Most PT practices post ERA payments without reading the patterns underneath. Here's what your remittance data reveals — and what it's costing you.

Dr. Andrew O'DonnellPhD, LSSGB
CEO and founder of ClaimCode. Expert in insurance analytics, digital transformation, and business operations. Passionate about helping private wellness practices manage their revenue cycle with meaningful insights.
Ready to stop losing revenue to denied claims?
ClaimCode gives your billing team real-time claim visibility and AI-powered remediation guidance — at flat-fee pricing.
Get Early Access